Marketing effectiveness case study
Optimizing member outreach campaigns to improve health outcomes
The challenge
How does marketing impact member health?
Quality member care is a crucial part of the long-term success of healthcare payers. Better member health outcomes mean healthier members, lower medical costs, less member disenrollment, improved Medicare Advantage star ratings, and bonus government reimbursements.
A Fortune 50 healthcare payer invested hundreds of thousands in outreach campaigns that asked targeted members to complete certain preventive screenings, aiming to improve overall member health outcomes. However, the ability to measure the effectiveness of these marketing campaigns was a challenge.
There were two main pain points. First, the campaigns consisted of multiple touchpoints across offline (direct mail, phone calls) and online (digital media) channels, making it hard to determine which tactics were driving preventive screenings. Second, the long-tail response curves of these campaigns and the time it took to receive claims data meant months of delay for analysis and optimization.
The objective
Optimize measurement efforts
This Fortune 50 healthcare payer wanted to develop a measurement plan to achieve three main objectives.
Determine Campaign Effectiveness
Are certain marketing campaigns effective in persuading members to take a test, get a screener or engage in other health outcomes?
Segment the Market
Which patient segments are responding to which marketing tactics and how do we capitalize on each using data?
Driving Continuous Improvement
How can the client infuse timely data-driven learnings into ongoing marketing cycles for continuous testing & learning?
The solution
Concurrent modeling and testing approach to measurement
Marketbridge solves the toughest marketing and sales challenges using quantitative, reproducible methods—and we have a history of helping healthcare leaders succeed in a crowded marketplace by optimizing channel coverage, personalizing the purchase experience, and measuring which marketing channels are driving results across the buyer journey. To accomplish this project, we leveraged all our experience and recommended a two-part measurement approach.
Build a Multi-touch Attribution (MTA) Model
A multi-touch attribution model (MTA) assigns fractional credit to each touchpoint in the gap closure campaigns. This allows the marketing team to see how much influence each channel has on a given member action.
Over the long-term, this type of member-level response analysis enables the marketing team to make marketing mix decisions across different member segments.
However, while an MTA model may at first seem to be an optimal solution, the response variable (in this case a member claim) takes several months to mature.
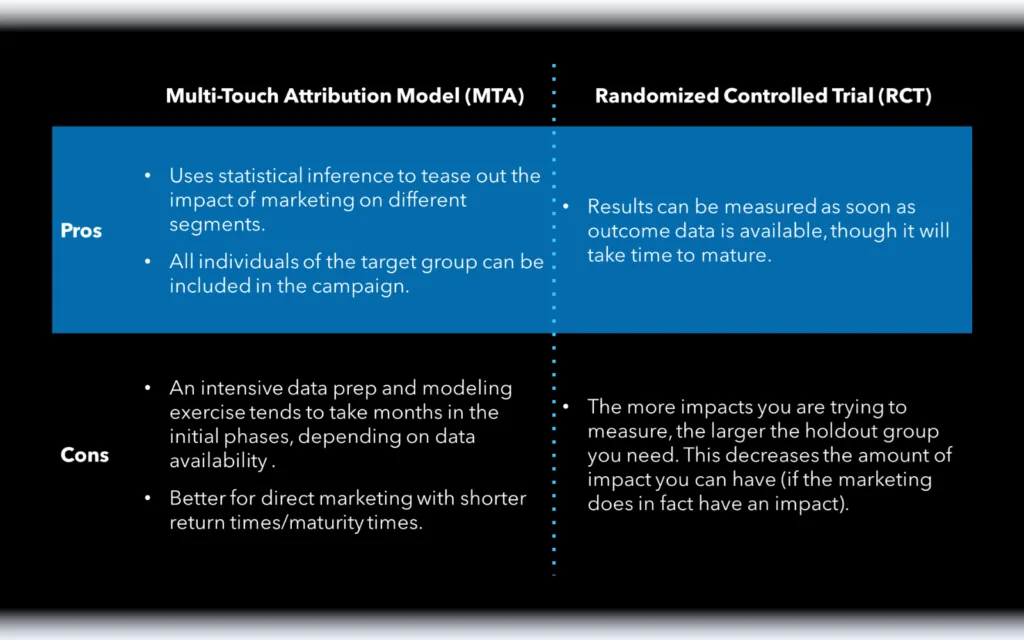
A response requires a member to schedule and attend an appointment, and the claim data has a time-lag. In this case, the long lead-time meant the model results would not be available until after the next year’s campaign planning.
To account for this delay, Marketbridge proposed pairing the model development with a Randomized Controlled Trial (RCT).
The RCT analysis proved that three out of four campaigns were successful in driving an incremental lift in gap closures. These timely results allowed the marketing team to optimize spend toward the three campaigns that were working, and bought time to “retool” the unsuccessful campaign for testing in a future campaign cycle.
As for the MTA model, the overall long-term results validated the findings of the RCT analysis and proved that most of the marketing campaigns were working.
However, to gain even more insight into how to best optimize marketing spend, Marketbridge applied an existing propensity model to campaign responders to see if marketing’s impact varied by a member’s “likelihood to close a care gap.” By looking at the results in this way, the payer learned the cost to market to each segment. As expected, members with a higher likelihood to close a care gap had overall lower cost-per-incremental-closure versus members with a low likelihood to close a care gap.
Business impact
Brand campaigns targeted at the right people led to improved marketing ROI
With our insights and recommendations, the client was able to increase their marketing ROI and optimize their budget to best improve overall member outcomes
Optimized Marketing Spend
Results showed that members with a higher likelihood of closing a care gap had lower cost-per-incremental-closure, leading the marketing team to streamline efficient outreach.
Improved Member Health Outcomes
The marketing team proved the impact of targeted care gap campaigns on preventive screenings, improving member health outcomes.
Timely Test and Learn Cycles
An RCT approach enabled the marketing team to work around long-tail response curves to build data-driven campaigns for year-round learning and optimization of marketing outreach.